Rebound
- or -
On Flaking Again
by Ed Dewke
I’ve got psoriasis. All over.
In my hair, on my butt, on my arms and legs, fingernails and feet, in my
ears. At the moment I don’t have any lesions visible on my face, though
there may be some beneath my beard. I’ve got a type of psoriasis lesion
on my scrotum and my penis.
I’m able to look a stranger in
the eye only because I wear clothes that cover nearly all of it. My
fingernails I don’t hide. People see them and think what they will.
Strangers don’t usually look in my ears. If I leave my scalp alone —
don’t scratch loose the flakes — and brush off my shoulders often, my
scalp P isn’t noticed, either.
Oh. I use the single letter “P”
to mean psoriasis when I write about this. Someone once commented, in
reference to an earlier essay of mine, “Aren’t you afraid that as people
read ‘P’-this and ‘P’-that they might be thinking of ‘pee’
as in piss?” He had a point, so I reread that essay, replacing the letter
“P” in my mind’s ear with the word “piss.” And you know what? It still
made sense — though the “piss” version was actually milder-feeling than
the intended meaning of “P” as psoriasis. I was surprised by this,
but shouldn’t have been. Everybody who has psoriasis knows it’s a real
pisser.
*****
Though I’ve had P for 16-or-so
years now (first diagnosed in 1990), I got rid of the symptoms on and off
starting in 1999. That was when I started using systemic medicines.
These are drugs that work from the inside out; taken as pills or shots.
Before that I was using topical medications — creams, ointments, lotions —
goops of various kinds. Several of them helped, but the symptoms
never went entirely into remission until I started the systemics.
 I’ll
never forget the feeling of being totally rid of my P symptoms. I feel
odd to write that because over the past seven years I’ve lived three or
four years symptom-free and, truth is, I did forget the feeling — and
pretty quickly, too. The change back to normal skin, in a psychological
sense, happened almost over night. We are comfortable in our normal,
lesion-free skin, so what’s remarkable about getting it back fades
quickly. After a couple of days of looking for lesions and not finding
any, I was mentally done with P. Ready to forget about it. It had all
been a bad dream. I think that unforgettable joyous feeling was
short-lived and probably occurred just prior to the disappearance of the
last visible lesion. I think I
looked at some previously lesion-infested part of myself, noticed how much
improved I was, and became aware that in a few days I might be completely
clear. THAT caused the joyous feeling. ANTICIPATION of
IMMINENT CLEARANCE. I’ll
never forget the feeling of being totally rid of my P symptoms. I feel
odd to write that because over the past seven years I’ve lived three or
four years symptom-free and, truth is, I did forget the feeling — and
pretty quickly, too. The change back to normal skin, in a psychological
sense, happened almost over night. We are comfortable in our normal,
lesion-free skin, so what’s remarkable about getting it back fades
quickly. After a couple of days of looking for lesions and not finding
any, I was mentally done with P. Ready to forget about it. It had all
been a bad dream. I think that unforgettable joyous feeling was
short-lived and probably occurred just prior to the disappearance of the
last visible lesion. I think I
looked at some previously lesion-infested part of myself, noticed how much
improved I was, and became aware that in a few days I might be completely
clear. THAT caused the joyous feeling. ANTICIPATION of
IMMINENT CLEARANCE.
Like I said, the actual
celebration was briefer than brief. Oh. All my lesions are gone. Did
I really live through that?
And the longer the remission
lasted, the further away I became, consciously, from any flaker’s
reality. The memories gathered dust and cobwebs. I forgot what things
were called — types of lesions, names of meds and procedures. I forgot
about the hours used up putting on meds, undergoing therapies; the pain
caused when water touches fresh cracks in the skin; bloody bed sheets and
underclothes; the flaky buildup on everything I touched, sat on, typed
on. I wonder if criminals just released from long prison sentences
experience anything like this? Did I just spend fifteen years in
prison? Oh yeah. Psoriasis. I had that once. Awful stuff, if I
remember correctly. I think the shrinks calls this “repression.”
And then comes the day the
now-normal flaker, the person who doesn’t think about P anymore — hasn’t
thought about it for months — unconsciously raises a hand to his scalp and
starts to scratch. A nail catches on something. It is a tactile
sensation you would have never thought about again — but the instant you
experience it, everything comes back. You are Cinderella at the Palace
and the clock has just struck midnight.
Oh. Shit.
You tug and the thing breaks
free. To the fingertips it feels like a dry scab. It’s grown around a
hair, so it doesn’t just pop out in your hand. You have to work it up and
off the hair shaft — easy or hard, depending on how long and curly your
hair is. It pops free, finally, but instead of catching it in the palm of
your hand it flies off somewhere. You gasp. Where the hell? And
— you’ll laugh about this later — you are rearranging things on your desk,
looking, and searching the carpet on hands and knees. Why? You’ve seen
these scalp flakes a million times. What’s the fuss?
At first, after the initial crash
and “oh shit,” there is a period of hope. This is a fluke, a rash, a
little allergy outbreak. Sufficient to yank me out of hubris but
nothing to panic about. Somewhere buried on a shelf in the bathroom there
must be a half-used bottle of that coal tar shampoo I used to use. What
was it called? Just look for the white plastic bottle with motor oil in
it.
 There
are fast and relentless rebounds that lay some people up. There’s a
psychological component, to be sure, but there’s probably a very real
physical component, too. Suddenly and fast you’re burning hundreds of
calories a day to make extra skin. It can sap the energy out of you.
People stay in bed, sleep twenty
hours at a time. Wake up feeling like they’ve been baked in a pottery
oven and will crack if the slightest breeze passes over them.
They’ll try anything to go back to sleep. (For too many years my antidote
and sleep inducer was Bombay gin.) There
are fast and relentless rebounds that lay some people up. There’s a
psychological component, to be sure, but there’s probably a very real
physical component, too. Suddenly and fast you’re burning hundreds of
calories a day to make extra skin. It can sap the energy out of you.
People stay in bed, sleep twenty
hours at a time. Wake up feeling like they’ve been baked in a pottery
oven and will crack if the slightest breeze passes over them.
They’ll try anything to go back to sleep. (For too many years my antidote
and sleep inducer was Bombay gin.)
When flakers experience what we
call a rebound, their P is rebounding from being suppressed by something.
The language here is deceptive. Suppressed P is a good thing. It means
your lesions are gone for awhile and your skin is normal or nearly so.
For some flakers, periods of suppression come without drugs or therapies.
Sometimes they come predictably, like during the summer if sun suppresses
your lesions and you have the inclination and time to soak up enough of
it. I think rebounds might not be so horrible for people who experience
predictable remissions. Mainly I think this because the rebounds
themselves are so predictable — as much so as the remissions. (People
I’ve heard from who look forward to summer and their skin clearing are
well aware of the fact that Fall means another relapse.) In fact, another
word is frequently used to describe these predictable rebounds:
FLARES.
“Flare” can mean any period of
unusually aggressive lesion formation. This can be as predictable as the
coming of cooler weather (and less sun) in the Fall, or “flare” can mean
the vicious onset of lesions when a drug therapy is stopped. Usually,
though, those vicious onsets brought on by ending therapies are referred
to as rebounds, especially if the therapy had been very successful in
making the P go away.
And that brings me back to
defining my P-life for the past seven years. As I mentioned, I’ve been
using systemic meds to combat my P since 1999. My history with flares
ended that year and my history with rebounds began. (Although I didn’t
really rebound until 2000 when my first systemic med decided to quit
working.)
*****
When I try to be analytical about
this disease, it helps me to think mathematically.
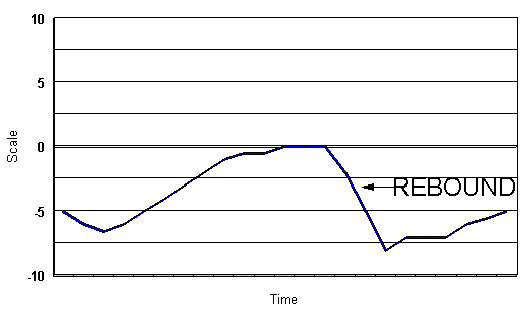 Imagine
a vertical scale (goes up and down, not side to side) that goes from -10
(minus ten) at the bottom to +10 (plus ten) at the top, with 0 (zero) in
the middle. A horizontal line to the right of this vertical scale starts
somewhere on the scale and moves up or down as time passes from
left to right. The zero mark is “normal skin.” This doesn’t mean perfect
skin. Perfect skin is +10 and usually obtained only in airbrushed
photographs. No, 0 skin is skin that’s got no problems, even though it
may have scars, stretch marks, freckles, “beauty spots,” etc. People live
comfortably at the 0 mark on the scale. Often, when they’re newborns,
they’re close to +10. Is there anything lovelier than a baby’s normal
skin? The way it feels and smells and glows under light? That’s what I
mean. By the time you are a toddler your score has probably dropped at
least half way down the scale to +5. Unless you’re a perfectionist that
spends lavishly on your skin, you may settle into adult life scoring 0 to
+1 or +2. (You get warts, calluses, bunions, boils, pimples, rashes...)
There are periods — usually brief in the overall scheme of things — when
your skin condition may dip BELOW zero. You may have a nasty dermatitis;
teenage acne; skin conditions derived from other underlying diseases. At
some point or another, probably everybody dips below 0 on the scale.
That, as they say, is life. Imagine
a vertical scale (goes up and down, not side to side) that goes from -10
(minus ten) at the bottom to +10 (plus ten) at the top, with 0 (zero) in
the middle. A horizontal line to the right of this vertical scale starts
somewhere on the scale and moves up or down as time passes from
left to right. The zero mark is “normal skin.” This doesn’t mean perfect
skin. Perfect skin is +10 and usually obtained only in airbrushed
photographs. No, 0 skin is skin that’s got no problems, even though it
may have scars, stretch marks, freckles, “beauty spots,” etc. People live
comfortably at the 0 mark on the scale. Often, when they’re newborns,
they’re close to +10. Is there anything lovelier than a baby’s normal
skin? The way it feels and smells and glows under light? That’s what I
mean. By the time you are a toddler your score has probably dropped at
least half way down the scale to +5. Unless you’re a perfectionist that
spends lavishly on your skin, you may settle into adult life scoring 0 to
+1 or +2. (You get warts, calluses, bunions, boils, pimples, rashes...)
There are periods — usually brief in the overall scheme of things — when
your skin condition may dip BELOW zero. You may have a nasty dermatitis;
teenage acne; skin conditions derived from other underlying diseases. At
some point or another, probably everybody dips below 0 on the scale.
That, as they say, is life.
But not for people with moderate
to severe P. For us, life is as close a niche to 0 as possible,
but nearly ALWAYS on the negative side of the scale (i.e., under
the 0 midway point). Our skin isn’t normal. It’s worse than normal, even
if strangers don’t notice. We yearn — no, we lust — for life at
the 0 level. Just give us normalcy! Live long enough at levels
well under 0 and you won’t care if you don’t stand-out on the beach as a
cover model — you’ll be happy if you can just lay out on the beach without
standing-out at all.
Dermatologists categorize P as
mild, moderate or severe. We’re taught that the size of the palm of our
hand is equal to 1 percent of our skin. With that in mind, under three
percent of skin effected is considered “mild,” 3%-10% is considered
“moderate,” and anything over 10% is considered “severe.” And, yes, I’ve
stood in front of a mirror and, with the help of my wife, “palmed over” my
lesions to come up with an approximate percent of coverage for me.
Without being specific, let me just say that qualifying in the “severe”
category has never been a problem for me during a flare or when I’m
rebounding.
When I’m feeling analytical, I
flip the doctor’s definition of mild, moderate or severe, so instead of
being 0% to 100% it becomes 0 to -10 on my scale, and then I can lay in my
own life-with-P line under the 0, depending upon how many lesions
are active at any given time. Since you already know my case is “severe,”
you could call me a “deep water dweller” most of the time, dragging my
line well below 0, which would be the surface in this mathematical
body-of-water-metaphor.
*****
Being equipped with this
analytical graph is well and good, and when I’m doing well on a systemic
treatment and can see that line climbing close to 0, I get to experience
that joyous feeling I mentioned some time ago. And it’s kind of geekishly satisfying to one day hit the 0 line (even if that’s the highest
you ever get to go). But the analysis has some problems.
The line you actually travel over
time might accurately display how you look — how much of your skin is
effected by P — but it doesn’t accurately reflect how you feel physically
or emotionally. This is because humans are a conscious species
with the ability to interpret real sensations and our feelings and
emotions are linked more closely to those interpretations than to
the reality in which we are immersed. Take for example the concert
pianist with P on her hands and fingernails. Those may be the ONLY places
she has P — putting her solidly in the “mild” category, mathematically. I
have heard about one musician who was near suicidal and ready to ditch a
brilliant career because of her hand/nail P.
There are kinds of psoriasis, and
places where psoriasis can show up on your body, that hurt more than other
places. If you have few lesions, but they are of this type or in those
places, the “mild-moderate-severe” categorization is insufficient.
*****
 There
are some pretty bad descriptions of P perpetuated in books and in
cyberspace, but the one I most loathe is the assertion that “psoriasis
lesions don’t itch.” If you haven’t come across this assertion,
you will. If I ever find its author I’m going to break his nose. There
are some pretty bad descriptions of P perpetuated in books and in
cyberspace, but the one I most loathe is the assertion that “psoriasis
lesions don’t itch.” If you haven’t come across this assertion,
you will. If I ever find its author I’m going to break his nose.
The problem with saying
“psoriasis lesions don’t itch” is it makes that fact universal therefore
untrue. (Even the derivation of the word is contrary to this assertion,
as it comes from the Greek word meaning “to itch.”) If the statement
were, “some psoriasis lesions don’t itch,” or “sometimes psoriasis lesions
don’t itch,” or any variation on either of these, it would be true and we
all know it. If all P lesions itched all the time, the disease would be
fatal. We’d all have scratched ourselves to death long ago.
Truth is, P lesions can and do
itch and, if I may be so bold, the ubiquity and severity of itch can be
classified as mild, moderate or severe. Not only do they itch, plaque
type lesions can crack and bleed — seemingly spontaneously — and get
infected. The huge debris fields that are, in fact, plaque lesions —
thousands upon thousands of hastily created dermis cells replaced
prematurely and stacking like leaves in the Fall — maintain some modicum
of adherence for quite awhile, meaning they stick to the living
skin, which is why plaque lesions get thick and the scales can clump
together so they peel off in sheets rather than scatter like dander. Look at a plaque lesion under a powerful magnifying lens and what itches
becomes apparent. The upper-most cells in the stack are being nudged and
pushed this way and that, creating a very rough surface that is
different than the healthy skin outside the lesion. This difference
is felt as “itch” when fabric rubs the skin, when a breeze moves the hair
that’s trying to survive in the debris field, when liquids saturate the
scale — or not. Point is, some lesions itch, some don’t. Some lesions
itch so bad it makes us cry. Or, more likely, we respond by scratching
and what happens then — How do I put this?
Oh shit2 (that's "oh
shit"-squared).
*****
Scratching is the worst possible
thing to do to a P lesion. It literally adds injury to insult.
A P lesion is an immune system
mistake, according to current medical convention. (There ARE theories
that offer alternatives to this.) Where there’s a lesion the skin is
behaving as though it was wounded. It has shifted into skin growth
overdrive and skin cells are being replaced faster than they die off and
get shed. Scratching in this particular battlefield tends to damage the
hyperactive skin, hence reinforcing the initially imaginary response to
damage and continuing that response. In other words, a scratched lesion
won’t get better. It will either stay the same or get worse.
So, itching a lesion isn’t just
an annoyance it is a very real threat to your skin. It never helps and it
can cause some serious hurt.
Which begs the question: Just
how bad can P get?
*****
Answer: Pretty damned bad. You
can get a lot of lesions (so many you look back at 10% coverage and laugh)
or the few lesions you do have can become infected. Either situation is
bad.
 Every
now and again some jerk in the midst of his 15 minutes of fame spouts that
psoriasis is a “cosmetic condition.” Literally that makes no
sense, because “cosmetic,” when used as an adjective, suggests to increase
attractiveness or beautify. But in this case “cosmetic condition” uses
“cosmetic” as an antithetical trope, for a malevolent reason. It suggests
the condition only adversely affects appearance; therefore P is not
dangerous or worthy of the same level of consideration as might be
received by cancer, asthma or multiple sclerosis. Talk about a pisser!
E.g., Why should we fund research to find a cure for psoriasis when it
is merely a cosmetic condition? These jerks can take my cosmetic
condition and stuff it where the sun don’t shine. Every
now and again some jerk in the midst of his 15 minutes of fame spouts that
psoriasis is a “cosmetic condition.” Literally that makes no
sense, because “cosmetic,” when used as an adjective, suggests to increase
attractiveness or beautify. But in this case “cosmetic condition” uses
“cosmetic” as an antithetical trope, for a malevolent reason. It suggests
the condition only adversely affects appearance; therefore P is not
dangerous or worthy of the same level of consideration as might be
received by cancer, asthma or multiple sclerosis. Talk about a pisser!
E.g., Why should we fund research to find a cure for psoriasis when it
is merely a cosmetic condition? These jerks can take my cosmetic
condition and stuff it where the sun don’t shine.
Has anybody died from P? I’m
told there have been deaths. I’m told erythrodermic psoriasis can kill
you. This is commonly defined as intensely inflamed lesions over large
areas. Sometimes it’s “full body.” It’s hard for me to imagine, but I
have corresponded with FlakeHQ readers who have “been there, done that.” This kind of P can lead to fatal dehydration (among other fatal things). Most of us won’t ever experience P this bad.
Which means our P must be
a cosmetic condition.
Okay, I’m done with that.
*****
 I
started this essay a month ago and now my editor (who, regrettably, is me)
is saying it’s time to wrap it and post it. There were a lot of other
things I wanted to write about. I
wanted to talk about the assortment of medicines and treatments I’ve
slathered on, ingested, injected, endured or embarked upon. When
you stop and think about our concept of “modern medicine” — an industry of
answers, health, longevity, cures, wellness and countless other words —
what we flakers have experienced until very recently was downright
laughable. You could never say to a flaker, “Use this and get well.”
(Saying anything remotely like that meant you were a snake oil salesman.)
No, the best you could say honestly was, “This works for some people.
Have you tried it?” We think the reason why palliatives and therapies for
P have performed so poorly is we haven’t understood the disease. We’ve
been concentrating on what’s visible about the disease, but the underlying
cause of the disease has evaded us. I
started this essay a month ago and now my editor (who, regrettably, is me)
is saying it’s time to wrap it and post it. There were a lot of other
things I wanted to write about. I
wanted to talk about the assortment of medicines and treatments I’ve
slathered on, ingested, injected, endured or embarked upon. When
you stop and think about our concept of “modern medicine” — an industry of
answers, health, longevity, cures, wellness and countless other words —
what we flakers have experienced until very recently was downright
laughable. You could never say to a flaker, “Use this and get well.”
(Saying anything remotely like that meant you were a snake oil salesman.)
No, the best you could say honestly was, “This works for some people.
Have you tried it?” We think the reason why palliatives and therapies for
P have performed so poorly is we haven’t understood the disease. We’ve
been concentrating on what’s visible about the disease, but the underlying
cause of the disease has evaded us.
(Of course, there are a lot of
advocates of a lot of therapy options that claim they DO KNOW the cause of
P, and their certainty about that CAUSE is supposed to validate their
therapy. In my personal opinion, many of these options are partially
right — right enough to help some flakers. But for me
there’s usually a looming question or two that isn’t answered to my
satisfaction....)
I wanted to write about current
research “clues” that suggest deeper understanding of P. Well after I
started this essay, Drea Garza, a member of PsorChat (http://health.groups.yahoo.com/group/PsorChat/message/4993)
brought our attention to an article from the National Institutes of Health
—
“Genetic Finding Suggests Alternative Treatment Strategy for Common,
Complex Skin Disorders and Asthma” — that contains some new thinking
about root causes of P (and other disorders).
(Actually, it’s not new
thinking. It’s already-thought-of-notions given new credence by a little
lab-based research.)
I find this stuff exciting. Even
when Big Ideas don’t seem to pan out (gene therapy, for example) I’m
excited. It represents a mark I can “x” out of my further consideration. (I, like most flakers, have x’d out more remedies than I care to
remember.)
Finally, I wanted to write about
what makes me survive my rebounds. When I started bouncing around the
palliative-and-therapy circuit looking for the perfect thing for me,
I’d occasionally leave something that was working in order to try
something else, in case it might work better, thinking if it didn’t I
could always go back.... Well, I’ve learned the danger of bouncing around
the palliative-and-therapy circuit is learning that you might not
be able to go back. It’s been my experience that, some times, you only
get one shot at relief. If you let the palliative that’s working for you
go, it may or may not work for you again, later. (The biggest “go
back” disappointment for me has been methotrexate, a systemic medicine
that, first time around, helped my P significantly but has, subsequently,
never been as effective as the first time.)
You’d think, having learned that,
I’d stop bouncing around. I know that when I stop something and then
start something uncertain I might experience a hideous rebound (like the
one I’m enjoying right now, triggered by stopping Raptiva [a biologic med]
to start Humira [another biologic]) so why do I risk it?
*****
I think I risk these rebounds in
my effort to reach “Zero” and stay there. Remember my graphic? The
minus-ten/plus-ten vertical axis and time being the horizontal access,
with 0 in the middle representing “normal” skin? Remember how I said few
people have +10 skin (mostly babies), but people without skin “conditions”
are mostly above zero while flakers are definitely below zero?
(What the hell am I talking about? If you need to, click
here to go back.)
Like I said, life at “0” — if I
can remember it — is mentionable because it is unremarkable. Being P-free
isn’t joyous, it’s normal. The thought of being P-free is joyous; knowing
when you are almost P-free, and that you are probably going to be
P-free soon, is joyous. But once you really reach 0 — your skin returns
to normal — the joy quickly fades and even memories of how bad it had been
tend to fade. Normalcy, like I said, is unremarkable. Beyond what may be
required to maintain your 0 state, you simply quit thinking about your
skin.
Granted, some people may set
their sights higher. They may want better than normal skin. They
want to climb past 0 on the scale — get tanned, wear thongs and draw
envious stares. Nothing wrong with that. I don’t set my sights higher
than normal because I’ve never really had better than normal skin, even
before I started to flake. I was subjected to lots of allergy-related
rashes as a child ... vitiligo set in with puberty ... melanin deficiency
meant I never could tan well.... I just want to float at 0 level. I may
or may not be happy there, but I know if I’m unhappy it won’t be because
of P.
At the moment, 0 is a long way
off. I don’t know if this rebound has reached its worst — I still have a
lot of lesion-free skin — and I don’t know what, if anything, will signal
the end of this rebound and the start of improvement. I’m waiting to see
if my insurance will cover doubling my Humira dosage. If I am allowed the
increased dosage, then I’ll have some additional number of months to wait
and see if that makes a difference. Meanwhile, P will rage on me and be
on my mind (and in my clothes, in my bed, on my floors, in my keyboard).
It will have an effect on my disposition and intellect that I am
impossibly positioned to appreciate objectively. I will be constantly
aware that 0 is a place I’ve been and a place I want to be again.
And I must laugh! I must laugh
because I know well that if and when I reach 0 again, I will forget, I
will purge myself emotionally of this awful rebound experience. I will
take my newly-achieved normal skin for granted. I will discover new
complaints that won’t have anything to do with my skin. I will joyously
anticipate reaching new goals that have nothing to do with flaking. So
that I don’t entirely forget, I may bury a copy of this essay in the very
back bottom of my sock drawer, where I may discover it years from now when
I’m at 0 or higher. And I will read it and wonder, Who the hell wrote
this?
-Ed
7/12/2006
Articles
www.flakehq.com |